
Read This Before You Confidently Get Abortion Wrong Again
How we let the stupidest ideologues frame the narrative & turn basic healthcare into a political battleground

Pro tip: Bookmark this article.
You will never again have to flail around, trying to think of how to answer one of these bad-faith quacks. This is your quick-reference guide for cutting through forced birth bullshit with facts — facts that center the patient, not the embryo.
But before we get into it, first, a vent about how we got here:
Nearly half the country has lost the right to bodily autonomy, and we have allowed this dangerous situation to become normalized.
I’m no longer screaming with frustration into the void about the GOP’s horrendous human rights abuses wrapped in banal legal briefs. I’ve finally accepted something pretty sobering: For much of the country, the loss of reproductive rights has become background noise — an abstraction rather than an emergency.
I’m not happy about it, of course, but there’s a certain relief in accepting that for many, this crisis only becomes real once it reaches their own body.
Brief Reminder About What Led Us Here
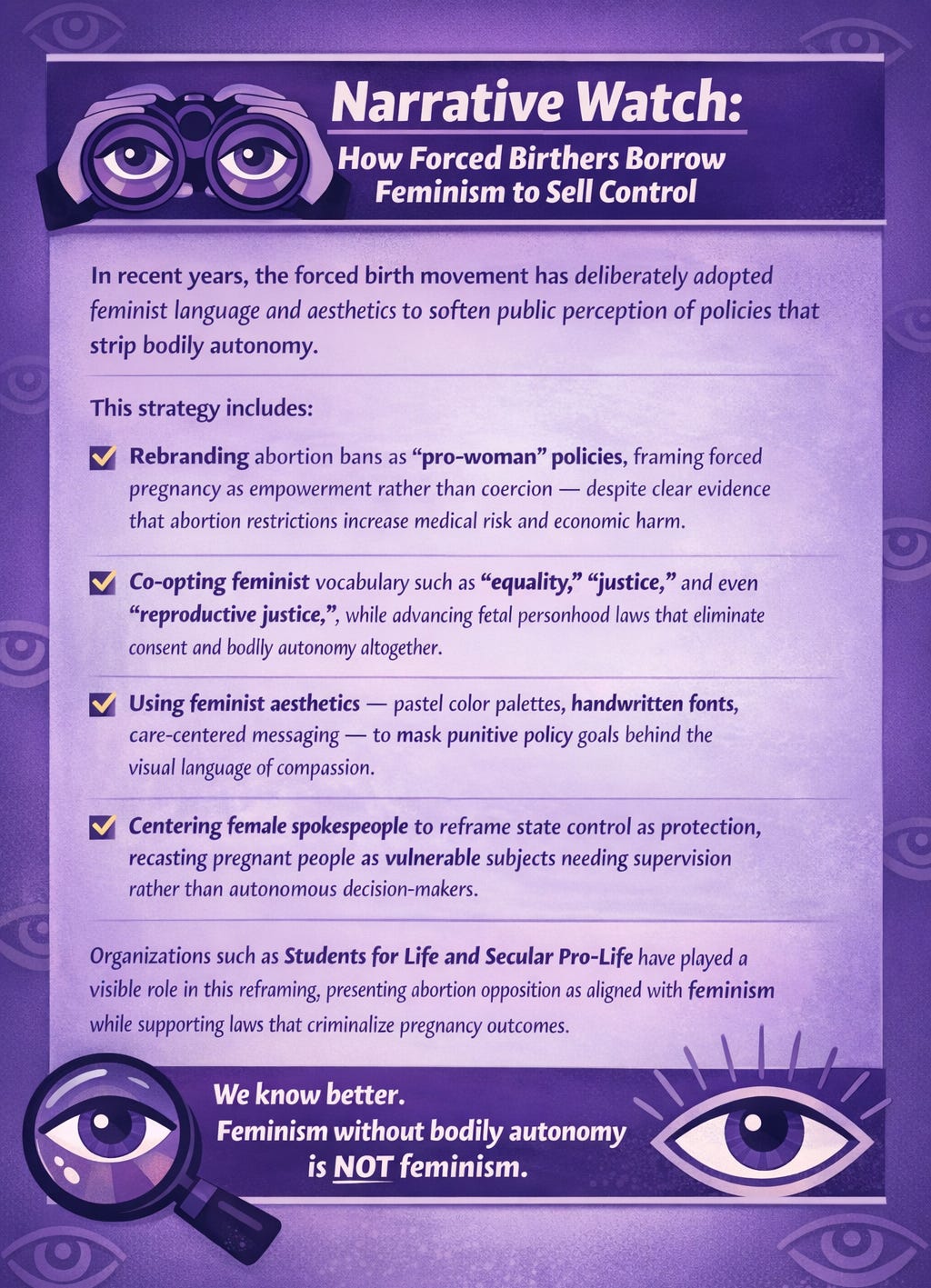
This didn’t happen overnight. The forced birth movement has spent decades capturing the narrative — framing the debate, controlling the language, lulling the media into a false equivalency, and shifting moral responsibility onto the very women, girls, and other pregnant folks harmed by its policies.
Institutional guardrails have failed. Political parties, corporate media, and professional gatekeepers have repeatedly declined to draw clear lines between evidence-based medicine and ideological extremism.
Misogyny has long been baked in. The United States has always operated as a patriarchy, with centuries of laws reflecting suspicion and fear of women’s autonomy — especially when it comes to reproduction.
Both major parties bear responsibility. Years of Democratic timidity, reflexive decorum, and a preference for fundraising and norm-preservation over a direct challenge has enabled Republican lies, aggression, and extremism.
The following video excerpt marks the moment in 2009 when Barack Obama reneged on another campaign promise and threw millions of American women under the bus (so he could prioritize slapping his name on a shitty, half-assed privatized healthcare bill):
“Both-sides” media framing has normalized extremism. Corporate outlets have treated religious ideology as just another viewpoint, describing abortion bans rooted in theology as merely “controversial” — instead of racist, classist, and deadly — while framing evidence-based healthcare as a matter of opinion.
Ideology has been laundered as medicine. Anti-abortion physicians spreading religiously motivated misinformation have rarely faced consequences and have formed parallel institutions designed to mimic legitimate medical authority and confuse lawmakers and journalists.
Healthcare has been politicized beyond reason. Elected officials with no medical training have dictated clinical care; prosecutors have second-guessed miscarriages; patients have been forced to prove their suffering is “innocent” enough to deserve treatment.
Even resistance has been narrowed. In Texas, some plaintiffs harmed by abortion bans stopped short of challenging the bans themselves, arguing instead for clearer emergency “guardrails” — a sign of how deeply this framework has been normalized. (And they lost the case anyway.)
Good-faith advocates on social media have been boxed in. Many abortion-rights supporters have found themselves arguing inside rhetorical terms set by the forced birth movement, leaving stigma unchallenged, the fetus and “when life begins” centered, and false premises intact.
As a result of all of these problems, the public conversation has drifted away from bodily autonomy, medicine, public health — and reality itself.
🎶 Sidebar break — doobie doobie doo 🎶
OK, Let’s Get to the “Fun” Stuff, Colleen!
Below is a breakdown of the most common claims advanced by the forced birth movement, followed by what medical evidence, public health data, and decades of research actually show. My debunks are non-ideological, peer-reviewed, and grounded in clinical practice.
This analysis begins where medicine begins: with the pregnant person — her health, her autonomy, and her rights.

CLAIM #1: “Later abortions are done casually because women just want to kill their babies”
REALITY: This claim is especially gross, false, and craven. (And, frankly, bat-shit insane.)
This is one of the most dangerous, misogynist lies perpetuated by the Right and the forced birth movement, because:
These are the emergency pregnancies when prompt abortion care could mean literally life or death for the pregnant patient.
The GOP’s erroneous laws THEMSELVES delay women and girls from accessing abortion earlier.
Later abortions are very rare and are associated with:
Severe fetal anomalies
Serious threats to the woman’s health
Previously mentioned delayed access caused by racist, classist abortion restrictions themselves
Women do not carry pregnancies for months and then terminate “on a whim.” This narrative exists to dehumanize patients and obscure the real consequences of restrictive laws.
CLAIM #2: “Abortion causes mental illness, trauma, or lifelong regret”
REALITY: Abortion does not increase mental health disorders.
The most comprehensive research on abortion and mental health is the Turnaway Study, a decade-long longitudinal study conducted by researchers at the University of California, San Francisco. It followed nearly 1,000 women who either received wanted abortions or were denied care due to gestational limits.
The findings were clear:
Women who received abortions were no more likely to experience depression, anxiety, PTSD, or suicidal ideation than women who were denied abortions.
The most commonly reported emotional response after abortion was relief.
Women denied abortions experienced worse mental health outcomes, higher stress levels, and significantly greater economic hardship.
These findings align with the positions of major medical bodies. The American Psychological Association has found no causal relationship between abortion and mental illness. The American College of Obstetricians and Gynecologists affirms that abortion is safe and does not harm mental health.
What research does consistently show is that trauma is associated with:
Forced continuation of pregnancy
Economic instability
Intimate partner violence
Medical emergencies
State surveillance and criminalization of pregnancy outcomes
The distress often attributed to abortion is overwhelmingly linked to coercion, stigma, and punishment, not the medical procedure itself.
CLAIM #3: “Women use abortion as birth control”
REALITY: This claim has been unsupported by data and sustained by misogynistic assumptions.
According to the Guttmacher Institute, more than half of women who obtain abortions were using contraception in the month they became pregnant. Contraception fails. Bodies are not machines. And access to reliable birth control in the United States has been uneven, costly, and increasingly shaped by political decisions.
Large areas of the country have become contraceptive deserts — places where women lack reasonable access to affordable contraception due to clinic closures, insurance restrictions, pharmacy refusals, and state policies that defund family planning providers. According to Power to Decide, a national, nonpartisan nonprofit organization focused on preventing unintended pregnancy in the U.S.:
Right now more than 19 million women in need live in contraceptive deserts. They lack reasonable access to a health center offering the full range of methods. Deep in the heart of those deserts, 1.2 million women in need live in counties without a single health center that offers the full range of contraceptive methods. -
These gaps are not accidental. For years, Republican lawmakers have opposed funding for contraception, blocked comprehensive sex education, and targeted providers that offer both birth control and abortion care.
Abortion is healthcare — a medical response when prevention fails, when health risks emerge, or when circumstances change. The notion that women casually undergo expensive, invasive, and often stigmatized medical procedures “for convenience” is not supported by evidence.
International research further undermines the claim. A major analysis published in The Lancet, one of the world’s most respected peer-reviewed medical journals, found that abortion rates are lower in countries where abortion is broadly legal and contraception is widely accessible. By contrast, abortion rates are higher — and far more dangerous — in countries where abortion is restricted and birth control access is limited.
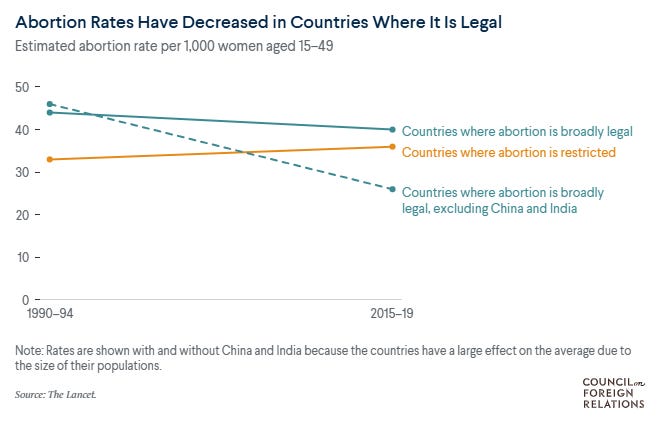
These findings are actually not counterintuitive. They reflect a consistent public health reality: when women have access to contraception, sex education, and healthcare, unintended pregnancies decline. Criminalization does not prevent abortion; it prevents safe abortion.
Taken together, the data make one conclusion unavoidable. The forced birth movement’s policy agenda has never been about reducing abortion rates. It has been about control — policing women’s sexuality, punishing pregnancy outcomes, and subordinating women’s autonomy to political power.
CLAIM #4: “Only liberal, leftist, ‘commie,’ ‘godless,’ Atheist women get abortions”
REALITY: Abortion has never been confined to a political party or religious identity.
Decades of data have shown that women who obtain abortions come from every political affiliation, faith tradition, income level, and geographic region. Large numbers identify as religious — including Christian — and many live in conservative states and communities.
You know why? Abortion care is not ideological — it’s a common healthcare decision shaped by pregnancy complications, economic circumstances, family needs, health risks, and life events that cut across belief systems.
Framing abortion as something only “liberal” or secular women choose has functioned as a political narrative, not a reflection of reality — one that obscures how widespread abortion care has been and how many women have been affected by its restriction.
CLAIM #5: “Abortion is more dangerous than childbirth”
REALITY: Pregnancy and childbirth carry significantly greater medical risk.
According to the Centers for Disease Control and Prevention, American College of Obstetrics & Gynecology, and other various studies, childbirth in the U.S. is much more dangerous and deadly than abortion.
Legal induced abortion is markedly safer than childbirth. The risk of death associated with childbirth is approximately 14 times higher than that with abortion. Similarly, the overall morbidity associated with childbirth exceeds that with abortion. - Obstetrics & Gynecology, 2012
The U.S. has the highest maternal mortality rate among peer nations due to a number of reasons, including:
A privatized, patchwork healthcare system
Inequitable policies
Maternity care deserts
And persistent systems of bias and discrimination across racial and ethnic groups.
Black Americans face a risk of pregnancy-related death two to three times higher than white women.
CLAIM #6: “Abortion harms women physically or causes infertility”
REALITY: Safe, legal abortion does not cause long-term physical harm.
Decades of medical evidence show:
No increased risk of infertility
No increased risk of breast cancer
No increased risk of complications in future pregnancies
The World Health Organization, the American College of Obstetricians and Gynecologists, the Centers for Disease Control and Prevention, the American Medical Association, the Royal College of Obstetricians and Gynaecologists in the UK, and the National Academies of Sciences, Engineering, and Medicine, all affirm that abortion is safe, does not cause long-term physical harm, and carries significantly lower medical risk than childbirth.
What does cause harm is delayed or denied care:
Being forced to carry non-viable pregnancies
Denial of miscarriage management
Fear of criminalization that deters women from seeking emergency care
These outcomes are direct consequences of abortion bans, not abortion itself. Yet forced birth organizations continue to use emotionally manipulative imagery and debunked claims to suggest danger where none exists.

Forcing or emotionally manipulating someone to remain pregnant against her will is not a neutral policy choice or “compassionate advice” — it exposes people to documented, preventable medical risk.
CLAIM #7: “Abortion bans protect babies”
REALITY: Abortion bans increase suffering and worsen outcomes.

States with the strictest abortion restrictions consistently show:
Higher maternal mortality
Higher infant mortality
Worse health outcomes for children
Fewer social supports for families
Abortion bans do not provide healthcare, reduce poverty, expand childcare, or support disabled children and their caregivers. What they do is expand surveillance of pregnant bodies, criminalize pregnancy loss, and entrench a punitive approach to reproductive healthcare. The GOP thinks this is gooooood policy.
CLAIM #8: “Abortion is immoral because it ‘severs dependency’”
REALITY: This argument fundamentally misunderstands bodily autonomy, consent, and what “dependency” means in law and medicine.

Bodily autonomy does not hinge on whether another being needs your body to survive. It hinges on consent. No person is legally required to use their body — organs, blood, tissue, or labor — to sustain another, even if refusal results in death. That principle applies universally.
Pregnancy is not a generic “dependency.” It is a uniquely invasive biological process that commandeers a person’s organs, alters the immune and cardiovascular systems, and carries significant medical risk. The law does not — and cannot — compel one person to undergo that level of bodily intrusion for another’s survival.
Forced-birth arguments often twist this distinction by invoking misleading analogies: breastfeeding, parental care, or “temporary support.” These comparisons fail because none of those involve involuntary use of internal organs. A woman can feed a baby formula. She cannot gestate a fetus without using her uterus, blood supply, hormones, and physical labor — continuously, for months.
Treating women like “life support” is dehumanization. It is a demand that women surrender bodily autonomy in a way no other class of people is required to do.
This is why bodily autonomy exists as a legal principle in the first place: to prevent the state from forcing people — especially women and girls — to function as biological resources for others.
CLAIM #9: “Abortion is murder; science says life begins at conception”
REALITY: This is a philosophical assertion, not a medical one.
Medicine does not define legal personhood. Science does not establish moral hierarchy. Biology does not confer citizenship.
What medical science recognizes is that pregnancy is a complex physiological process involving one existing person — the pregnant one — whose body bears the risk, labor, and consequences of gestation. A fetus is biologically dependent and cannot survive without another person’s body.
From a legal standpoint, abortion does not meet the requirements for “murder.” Criminal homicide requires:
Mens rea — a culpable mental state directed toward unlawfully killing a legally recognized person.
Actus reus — an unlawful act that causes that death.
Abortion involves neither, which is why forced birth arguments rely on redefining words rather than applying law. It is a lawful medical procedure performed with the consent of the patient, by licensed clinicians, without criminal intent, and without a legal duty to sustain another body.
Criminal law exists to limit state power, not expand it. Concepts like mens rea and actus reus ensure that punishment is based on intent and unlawful action — not moral belief or political ideology. Redefining medical care as “murder” by discarding these standards does not protect life; it dismantles the rule of law itself. And it is a threat to everyone.
There is no other context in law where one person is compelled to use their body to sustain another. If bodily obligation were a legal principle, organ donation would be mandatory. It is not — because bodily autonomy.
Just your daily reminder that your religion does not dictate the rules for OUR bodies.
CLAIM #10 (related): “Abortion is murder — otherwise, why is it double homicide when someone kills someone who’s pregnant?”
REALITY: These laws exist to protect pregnant women from violence — not to grant fetal personhood or redefine abortion as homicide.
So-called “double homicide” or fetal homicide laws were created to address violent crimes committed against pregnant women by third parties, most often intimate partners.
The legal distinction rests on consent
In cases of violent assault or homicide, a pregnant woman did not consent to being killed, nor to the loss of her pregnancy as a result of that violence.
Abortion, by contrast, is a consensual medical decision made by the pregnant person themselves. There is no violent assailant, no unlawful act, no mens rea to kill a legally recognized person, and no actus reus that constitutes criminal homicide. Treating these situations as legally equivalent erases consent, agency, and the purpose of laws designed to protect women from violence.
Crucially, double homicide laws:
Require a violent third party
Require lack of consent
Explicitly exclude abortion and medical care
Preserve the pregnant person’s autonomy
They are victim-protection statutes, not personhood statutes, and have nothing to do with “murder.” Once again, forced-birth rhetoric relies on redefining words to obscure reality.
But if fetal homicide/double homicide laws were truly about declaring abortion as “murder,” they would criminalize pregnant women. They do not — because doing so would violate foundational principles of bodily autonomy, due process, and medical decision-making.
Forced birth “logic”: Violence against a pregnant woman is treated as evidence that she must surrender control over her body. Are we seeing the pattern?
Speaking of patterns…
The Pattern and Context Behind the Claims
We have already seen this agenda in action. The Heritage Foundation’s Project 2025, embraced by the Trump administration, translated ideological goals into concrete policy shifts that reshaped federal governance around a narrow, traditionalist vision of family, pregnancy, and gender.
The framework treated abortion as outside the scope of healthcare, pushed agencies to emphasize “life from conception to natural death,” rolled back Title X family planning protections, defunded Planned Parenthood clinics that served as primary healthcare providers for many low-income communities, and revived attempts to apply the 19th-century Comstock Act to restrict mailing abortion medication.
More dangerously, Project 2025 informed executive actions that weakened protections for emergency abortion care under EMTALA, reaffirmed funding bans, and deprioritized reproductive health across federal agencies. At the same time, broader policy changes elevated “traditional family” structures while opposing sex education, contraception access, and gender-affirming care — a coordinated rollback of bodily autonomy across issue areas.
Enforcement has been conspicuously selective, of course. Anti-abortion violence continues to be treated as a secondary concern, while abortion-rights activists — particularly those who target crisis pregnancy centers — are singled out for punishment. Meanwhile, those centers have proliferated with public funding and legal protection, despite a documented record of medical misinformation and coercion.
And this has not stopped. We are only days into 2026, and the same priorities remain front and center: restricting contraception, pushing toward a national abortion ban, and using federal power to force women out of public life and back into compulsory motherhood.
By the end of 2025, much of this agenda was already completed. Now, in 2026, it is being expanded and enforced — with women, girls, and marginalized communities paying the price.
The Record Is Clear
There is no debate about our human right to bodily autonomy.
Abortion access is supported by every major medical authority and grounded in public health data, clinical practice, and decades of peer-reviewed research. It reduces harm, preserves life, and respects bodily autonomy.
We don’t let plumbers perform open-heart surgery — so there is no rational reason politicians should be dictating OBGYN care.
The Forced Birth Industrial Complex has had decades to produce evidence that abortion harms women or protects families. It hasn’t — because it can’t. Instead, it relies on misinformation, stigma, religious ideology, and the distortion of medicine and law, increasingly enforced through state power.
This is not a moral disagreement. It is a political project that uses coercion and surveillance to control women and girls.
We don’t need better slogans or another generation of polished nonprofits offering platitudes. We need to stop legitimizing claims that collapse under basic scrutiny — and consistently center the woman or girl whose body, health, and life are actually at stake.
Bodily autonomy is not a messaging strategy, and it is not up for debate with some bro on Instagram. It is a fundamental freedom — and it is being dismantled. Treat that with a lot more urgency.
Fueled by green smoothies and Gen X grit, Colleen Luckett is part literary witch, part intersectional feminist warrior calling out forced birthers, capitalist co-opters, and faux-feminists — strong-willed, justice-rooted, and done playing nice with fascists. Featuring Miscarriage of Justice, a series that brings you the receipts on the structural racism and misogyny, pervasive corruption, and weaponized stigma behind pregnancy criminalization. You can also find her on Instagram, TikTok, and YouTube, and listen to The Abortionfluencer Podcast wherever you get your podcasts.
Yep. And if pro-forced birth proponents want to call abortion “murder” I say “no, justified self-defense.” Pregnancy carries a non-trivial risk of death or disability. You have THE RIGHT to use deadly force against one who threatens your life, however unintentionally.
Here in kansas, we have a group called abolitionists rising, they bring big Sandwich board sized signs to clinics and prop them up so that cars can't get past without seeing them. I call the one with the big bloody fetus the magic gummy bear poster. They're also always paddling on about preborn children and how a fetus that is going to be a girl has ovaries and Fallopian tubes at X number of weeks gestation, as if they can't wait to start legislating those too.